You are probably wasting your time applying ice to that sprained ankle or inflamed tendon and possibly even doing it some extra damage.
Before I explain myself, a little history about ice therapy in NZ:
Back in the late '70's in my role as the ACC's National Coordinator of Sport and Recreation Safety, I attended a combined physiotherapy and sports medicine conference in Dunedin. The All Black's team physiotherapist, Peter Stokes, presented a paper on the the use of Ice, Compression and Elevation (ICE) for the first aid treatment of soft tissue injuries. I subsequently devised a public education campaign directed at sports coaches and sports people and this was delivered principally via the NZ Federation of Sports Medicine which had active branches throughout the country at the time. Back in those days, the treatment of choice was heat rub, massage and running the injury out. Much emphasis in the campaign was therefore placed on getting rid of these harmful practices. It was natural, therefore, to emphasise the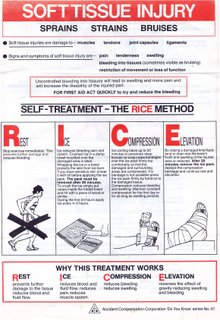 "I" in the ICE. As we all know what to do nowadays, I am proud to claim this campaign was obviously a huge success.
"I" in the ICE. As we all know what to do nowadays, I am proud to claim this campaign was obviously a huge success.
The brochure to the right is the front page of the original that I put together. Incidentally, the illustrations were done by nationally ranked middle distance runner, Alastair Leslie, who I was assisting with coaching at the time.
But does it work? The rest does (the elevation and the compression); but probably not the ice.
Before I explain myself, a little history about ice therapy in NZ:
Back in the late '70's in my role as the ACC's National Coordinator of Sport and Recreation Safety, I attended a combined physiotherapy and sports medicine conference in Dunedin. The All Black's team physiotherapist, Peter Stokes, presented a paper on the the use of Ice, Compression and Elevation (ICE) for the first aid treatment of soft tissue injuries. I subsequently devised a public education campaign directed at sports coaches and sports people and this was delivered principally via the NZ Federation of Sports Medicine which had active branches throughout the country at the time. Back in those days, the treatment of choice was heat rub, massage and running the injury out. Much emphasis in the campaign was therefore placed on getting rid of these harmful practices. It was natural, therefore, to emphasise the
 "I" in the ICE. As we all know what to do nowadays, I am proud to claim this campaign was obviously a huge success.
"I" in the ICE. As we all know what to do nowadays, I am proud to claim this campaign was obviously a huge success.The brochure to the right is the front page of the original that I put together. Incidentally, the illustrations were done by nationally ranked middle distance runner, Alastair Leslie, who I was assisting with coaching at the time.
But does it work? The rest does (the elevation and the compression); but probably not the ice.
- Rest - for about 36 hours ensures time to properly seal small blood vessels that have been disrupted.
- Compression - for about the same time prevents fluid, including blood from engorging the damaged tissue and joint spaces while the clotting process seals off the damaged blood vessels.
- Elevation - several centimeters higher than the heart will stop blood flow into the damaged area (The most effective way to stop a cut finger bleeding is to compress the cut and hold it above the head - try it next time).
Ice might reduce blood flow a little by causing a constriction of the blood vessels. But, cool the area too long and the opposite happens. Sure, cooling the area might marginally reduce the pain; but who cares! Acute pain has a purpose. Incidentally, compression is another means of dulling the pain. Ice applied to an area risks causing ice burns. I have seen many cases of ice burn and the damage can be serious in some cases. Some people have very sensitive tissue and are best advised to avoid ice therapy altogether. The consequence of excessive cold is SWELLING - the very thing the ice was applied to prevent! Pouring cold water on the injured part might seem safer; but the problem is the more important compression and elevation are probably not happening while this is being done and the injured body part will probably be well below the heart. Not good if the intention is to halt bleeding.
However; an ice pack consisting of crushed ice, or a packet of frozen vegetables wrapped in a damp towel, can make an effective pad for compressing a badly bruised or torn body part.
Never apply frozen things directly to skin, which is why we say that it must be wrapped in a damp towel. Remove the ice after about 5 minutes and continue the compression with a soft pad only that is held in place by firm, but not painful pressure by the wide pad of the hand and/or an elastic bandage that extends well above and below the injury site. Any bandages should not be so tight as to cut off circulation to a limb.
If, for example, you sprain an ankle; this is my recommended course of action:
- Stop and lie down - choosing the first available warm, dry place. You must keep warm
- Raise the ankle above body level asap
- Hold that position for up to 15 minutes (You need to give the damaged blood vessels time to seal with a blood clot before putting the leg down and moving about)
- If a compression bandage is available, apply this while the leg is elevated and use enough banadage to cover the whole foor to the toes and all of the bottom half of the lower leg
- After about 15-20 minutes, you can make the move to a more permanent place to continue the rest, compression and elevation for a few more hours.
- After about 36 hours and so long as nothing is broken, it is recommended that you start weight bearing and moving about, doing your absolute best to walk with the foot straight and without a limp.
- Continue the elevation and compression between exercise for as long as swelling is evident.
- If there has not been a significant improvement in pain and mobility within about 48 hours, you should think about getting on down to the emergency department or seeing your doctor, just in case you have broken a bone or popped a tendon.
- From about 72 hours, all going to plan, you can carefully and gradually resume normal activities.
Notes:
- If you feel a tearing or giving way sensation at the moment of injury or hear a popping or snapping sound, you may have ruptured an important structure that requires early treatment. This kind of injury can sometimes be deceptively painless at first. See your doctor asap and report what you felt or heard.
- Even if you think you might have done a serious injury, don't rush off to the emergency clinic. Stabilise the injury first by an hour or so of compression and elevation. Rushing around and then waiting for hours at the emergency clinic, to only be seen by a junior doctor, may be the worst thing you can do, possibly setting your recovery back by days, if not weeks. Ring the department and find out what is the best time to come in. You might even be better off booking in to see a General Practitioner with postgraduate training in sports medicine in a day or so.
- If it is an accident, then there is no excuse for getting medical help in countries like New Zealand, since most of the medical costs are covered by ACC or a similar agency.
2 comments:
Hi Gary
I would be very interested in finding research that has been done into the effectiveness of ice on soft tissue injuries. These injuries often happen to tennis players and ice is still the standard inital treatment. Is using ice your own preference or is there a body of research that backs this up? Terry
Terry,
There has been a lot of research over the years; but I do not know of any that actually answers your question. I think the respective benefits get confused. Applying ice packs always involves some compression and using aerosol sprays on skin is very risky if applied for more than a second or two and pouring water over a bruise or sprain is not very practical for more than a few minutes and may be negated by being unable to elevate or compress the area being watered.
As I said in my article, an ice pack is a good way to apply compression and the cold might help cut some bleeding over the first 5 or so minutes.
I think this might be partly a case of a Truism in operation - it has been said that "it is so" so many times by those in authority that people have not dared to question what is really working.
I feel the ice portion has been overly emphasised because of the original need to get rid of heat treatments that were in widespread use up until about 1980.
Terry: Try an experiment on yourself. Next time you race up to the net to do an overhead volley and go over on an ankle; try compression and elevation only and see what happens. Please report back to us when the experiment is complete, thankyou.
Post a Comment